Post infectious IBS
IBS cases in which symptoms emerged after an infection, most commonly gastroenteritis
Number of cases
Mean age
Rate of success
Treatment duration
Most common symptom
Most common culprit
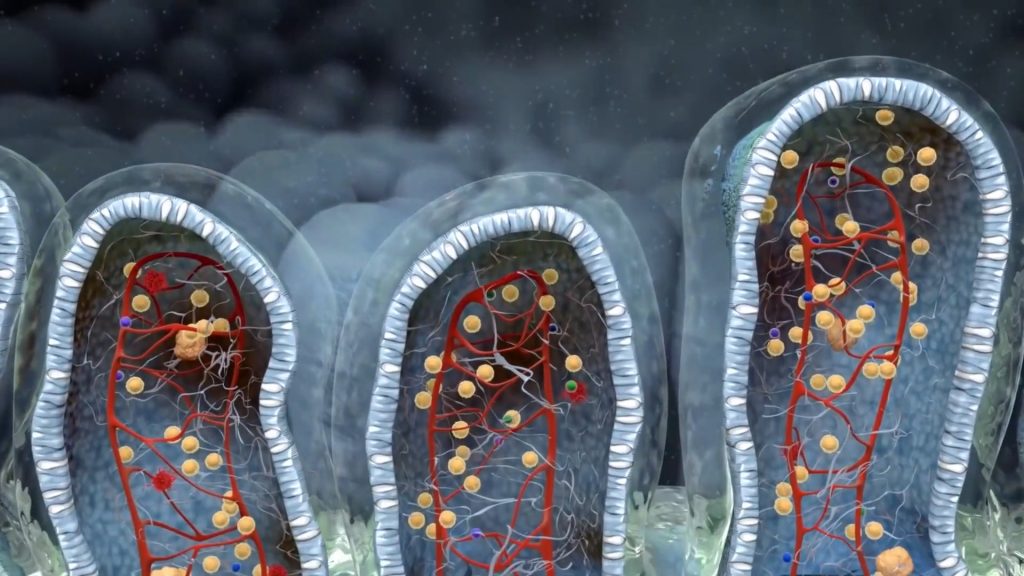
Most people suffering from any kind of irritable bowel syndrome are usually predisposed to it. Predisposition in IBS arises from a variety of factors, mainly nutritional, environmental, stressful, infectious and some genetic. These people may be at the edge of manifesting IBS for years before symptoms appear. The trigger that may bring their symptoms to the surface varies from case to case, with the most common of all being a bacterial, viral or parasitic infection. The intestinal mesh produced by the violent immune response against the infectious agent sets the basis for the onset of the syndrome.
It is the most common trigger of irritable bowel syndrome. When the intestinal environment is already vulnerable, a powerful infectious agent may cause significant changes in both the mucosal layer and the microbial ecosystem
Other infections, beyond the gastrointestinal tract, significantly affect the immune response and tolerance of resident gut populations. These include infectious agents like HIV, CMV, Epstein-Varr virus and many more
Emergence of irritable bowel syndrome symptoms after or during an antibiotic treatment is very common. Most of the times the damage is reversible, it dependes, however, on the chronicity of their use and the type of antimicrobial substances taken in the long run
Many patients report that their symptoms emerged after a traumatic event or a prolonged period of very intense stress. This can be attributed to the modification of the GI nervous system regulation, in order to adapt to the stress, making bowel movement more sensitive to even minor stressors. The vagus nerve is involved in this evolutionary critical process.
Radiation colitis is the most common complication of bowel and bladder cancer radiotherapy. In many cases it is not possible to regain full intestinal function
Chronic use of proton pump inhibitors inevitably leads to physicochemical alterations of the intestinal mucosa as well as to very intense microbial ecology perturbations
Some surgical operations, mainly involving abdominal areas, may lead to the creation of scar tissue and wrecking of local intestinal physiology. In addition, some reports blame anesthesia for inducing deleterious changes in the intestinal microbiome
Dental procedures are not rare triggers of IBS symptoms. Usually, this kind of IBS resolves on its own and probably the culprit is the antibiotics used after some dental procedures.
There are several other triggers reported from patients, like during and after traveling by airplane, after visiting places with very high humidity, after moving to a new house and more. Most of them eventually converge to one of the most common IBSyncrasies
Katie was a perfectly healthy woman who until she turned 39 years old, had no symptom of gastrointestinal origin. She reported that she would eat without any restrictions and never experience any problem. 2 years ago, after an evening scuba diving lesson, she returned home and, according to her report, she did not feel hungry as usual, so she just ate a yogurt. This was the last time she remembered being pain free. Several hours after eating the yogurt she started feeling a strange pressure around her belly button and a few minutes later she ended up having diarrhea. This symptom pattern insisted for 6 days. Within the next year she visited 3 MD’s, she was prescribed several treamtents and performed all kinds of tests, which all came negative. Taking into consideration that her mother had passed from colorectal cancer, she could not help thinking of a malignancy, although her colonoscopy was clear. The only thing that calmed her symptoms was loperamide (anti diarrhea agent) but she knew that this was just a symptomatic relief.
Alteration of microbiome balance pavew the way todistorted mucosal properties and antiboitics play a major role by enhancing dysbiosis
A well nourished microflora can handle parasitic infections and usually present with mild gastrenteritis-like symptoms. A predisposed gut, though, may suffer augmented damage
When the microbiome is already predisposed, mold can inhbit easily the intestinal environment and multiply faster
Parasites and bacteria that colonize the intestinal environment for longer than they should, start secreting substances that condition the environment to favor their growth, instead of commensal bacterial growth perpetuating IBS symptoms
The main aspects of Katie’s pathology needed investigation were smelly gas, epigastric pain, diarrhea and the long lasting burping incidents. All of them had a central cause and this was the deterioration of her microbiota (dysbiosis). Symptoms may, indeed, have been triggered by the spoiled yogurt she consumed, but the context this trigger took advantage of was the chronic dysbiosis attributed to the antibiotic abuse. Of course, I needed to exclude other, more serious causes, like adult onset celiac disease and sIgA deficiency.
The characteristic odor of gas produced by parasites or septic bacteria stems form sulfur and nitrogen convertion to hydroxen sulfide and ammonia, respectively
Constant diarrhea is usually more serious than episodes of diarrhea. The episodic nature of the symptoms is usually attributed to the ever changing microflora status
While burping is usually a stomach-derived symptom, in certain cases of IBS gas may leak from the large intestine, especially when small intestinal bacterial overgrowth is present
Residual feeling is usually false. That means that there is no residual fecal content inside the gut lumen, rather the inflammatory reactions against the chronic infectious agents, like Proteus, enhance the feeling of fecal material
This case is an excellent example of a patient whose mainstream diagnostic tests are negative but a wealth of findings is revealed by advanced biochemical and molecular testing. In fact, the only negative result I got from Katie’s results was the blood celiac disease test. Heavy dysbiosis, infectious inflammation, allergic mediators, malabsorption, even a parasite had set the stage for Katie’s pathology, and it was not a simple one.
Histamine produces anaphylactic-like reactions in the gut leading to diarrhea
D. fragilis is a constant eosinophil activator. EPX mediates allergic reactions both in the intestine and the circulation
This bacterium produces hydrogen sulfide which makes gas smell. In addition intermittent diarrhea may be exaggerated by its presence
Probiotic sterility leads to abnormal fermentation of starch, sugars and fiber. Bloating and gas are main symptoms
Katie’s case was not a simple one, due to the multitude of her findings. For this reason, her treatment had several stages, each one aiming at different aspects of her syndrome. The first stage targeted the parasite along with gut and stomach lining protection. Once parasite levels were reduced, it was Proteus time. Due to the fact that I would use an antibiotic for D. fragilis, I chose a plant based antimicrobial blend for Proteus, strong enough though. The last part of her treatment consisted of anti-inflammatory, anti-histamine and gut nourishing agents.
Two months later Katie walked into my office obviously content with the course. She looked better as she had regained the weight she had lost because of her bowel problem. Her diary was blank as her stools were now formed and gas was scarce, there was no burping after meals and her psychology was very good. I told her to repeat the last two months and to reassess several inflammation markers and a parasitology stool test.
Gastrointestinal infections have the potential to produce violent and long lasting reactions. These responses are very important as they serve a lifesaving purpose; to inhibit the passage of microbes or toxins inside the body. Their impact on gut physiology is great, but a healthy intestinal ecosystem can overcome this impact and restore its function.
In a compromised ecosystem, imbalanced microflora and downregulated immune barriers may not be able to overcome the infection, giving rise to long lasting post-infectious irritable bowel syndrome. While the case described above is a diarrhea-predominant one, many post-infection cases present with constipation.
Independently of the form the syndrome possesses, it is critical to identify the pathogenic bacteria overgrowth and the comorbid changes that have taken place because of the infection. Once this information is available, post infectious IBS can be cured, and it usually is. The patients need to be insistent and not give up after the first flare up. The infectious agent that caused the infection in the first place is not to be blamed for PI-IBS, it is the imbalanced microflora and gut-associated immune barriers that cannot prevent the outcome.
- Infections may trigger IBS but in order to do so other predispositions must exist. Heavy dysbiosis or immune downregulation are the most common commorbidities
- Irritable bowel symptoms usually take 2 to 3 months to resolve but a strong immune enhancing treatment must be followed for at least 6 months
- Diarrhea and bloating are the most prominent symptoms, whereas other symptoms like burping are common
- While our gut ecosystem has an incredible capability of self repairing, chronic assaults, like antibiotics and poor food choices may disrupt its balance
- Women are more prone to post infectious irritable bowel syndrome. It seems that some hormones make women more susceptible to dysbiosis